Our Research
Contact EHPL
Inquiries
Tel: 519-661-2111 ext. 80173
Email: hprapave@uwo.ca
Room 2107B, Thames Hall
Western University
London, Ontario, Canada
N6A 3K7
Lab Hours
We are currently operating on virtual office hours. Please email the person you need to contact or send your inquiry to hprapave@uwo.ca.
Past Projects
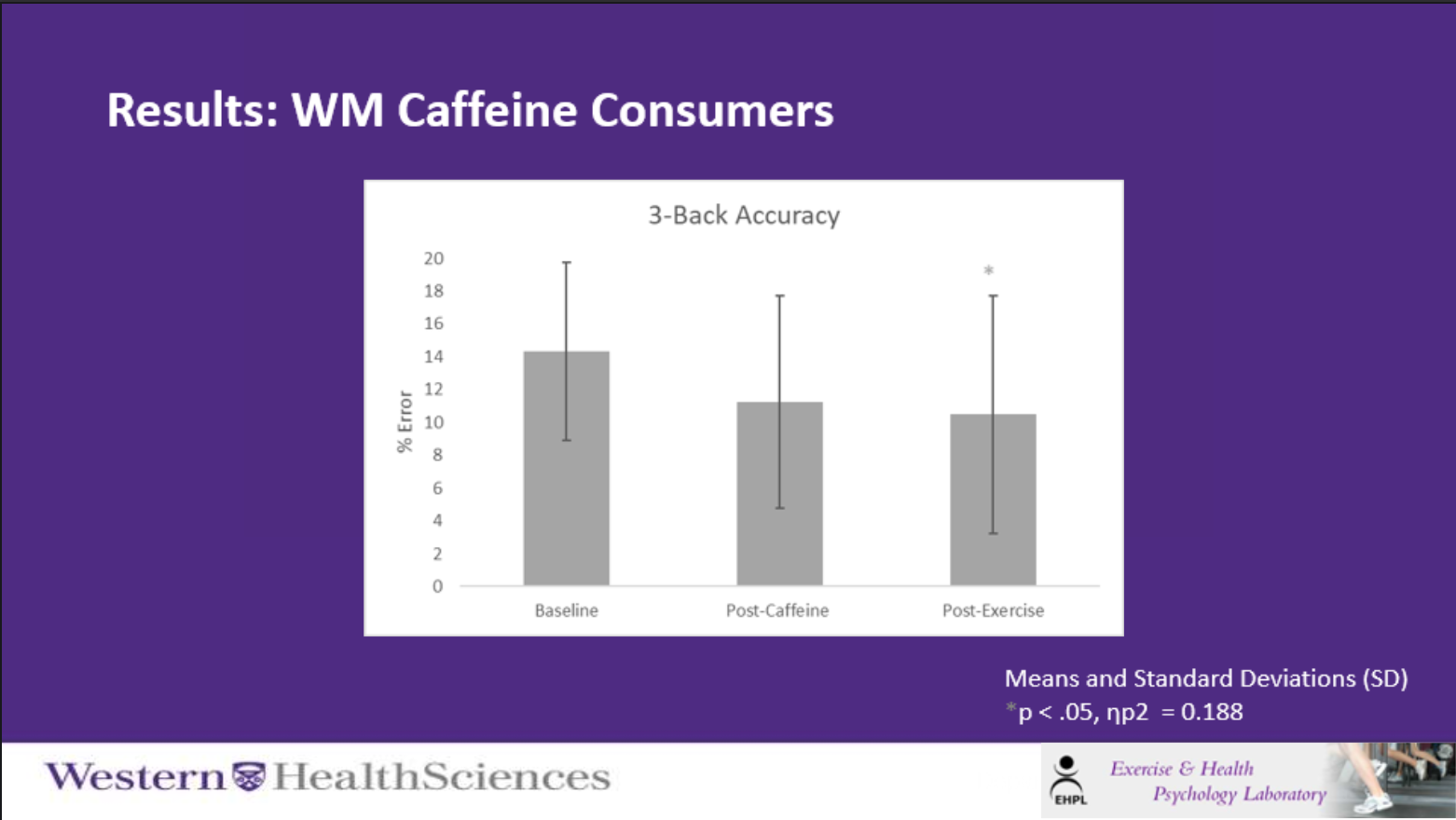
The Effects of Acute Aerobic Exercise and Caffeine on Working Memory
Anisa Morava
Caffeine is one of the most predominantly used psychoactive substances worldwide (World Health Organization [WHO], 2004). A primary motivator for caffeine consumption is its cognitive benefits (Temple, Dewey, & Briatico, 2010). Aerobic exercise has also been associated with numerous cognitive benefits (Chang et al., 2014). The effects of aerobic exercise in comparison to caffeine on working memory in both caffeine and non-caffeine models remain unknown. Caffeine consumers (<150mg/day) and non-caffeine consumers (<30mg/day) completed a baseline working memory assessment (n-back task, Owen et al., 2005) then participated in both an exercise and caffeine intervention in a counterbalanced manner. The exercise intervention consisted of 20 minutes of moderate intensity exercise (40-60% Heart Rate Reserve), while the caffeine intervention consisted of ingesting 1.2mg/kg of caffeine followed by the n-back task. N-back task performance was characterized by reaction times (milliseconds) and accuracy (percentage of errors). Preliminary analyses indicate caffeine consumers showed accuracy improvements post exercise (p <.05), while non-caffeine consumers showed accuracy improvements post caffeine (p <.05). Both caffeine consumers and non-caffeine consumers did not show a speed-accuracy trade-off as reaction times remained relatively stable, while accuracy improved. These results indicate aerobic exercise may pragmatically improve working memory in caffeine consumers. Further research should seek to elucidate the mechanisms underlying exercise-cognition interactions in relation to caffeine consumption.
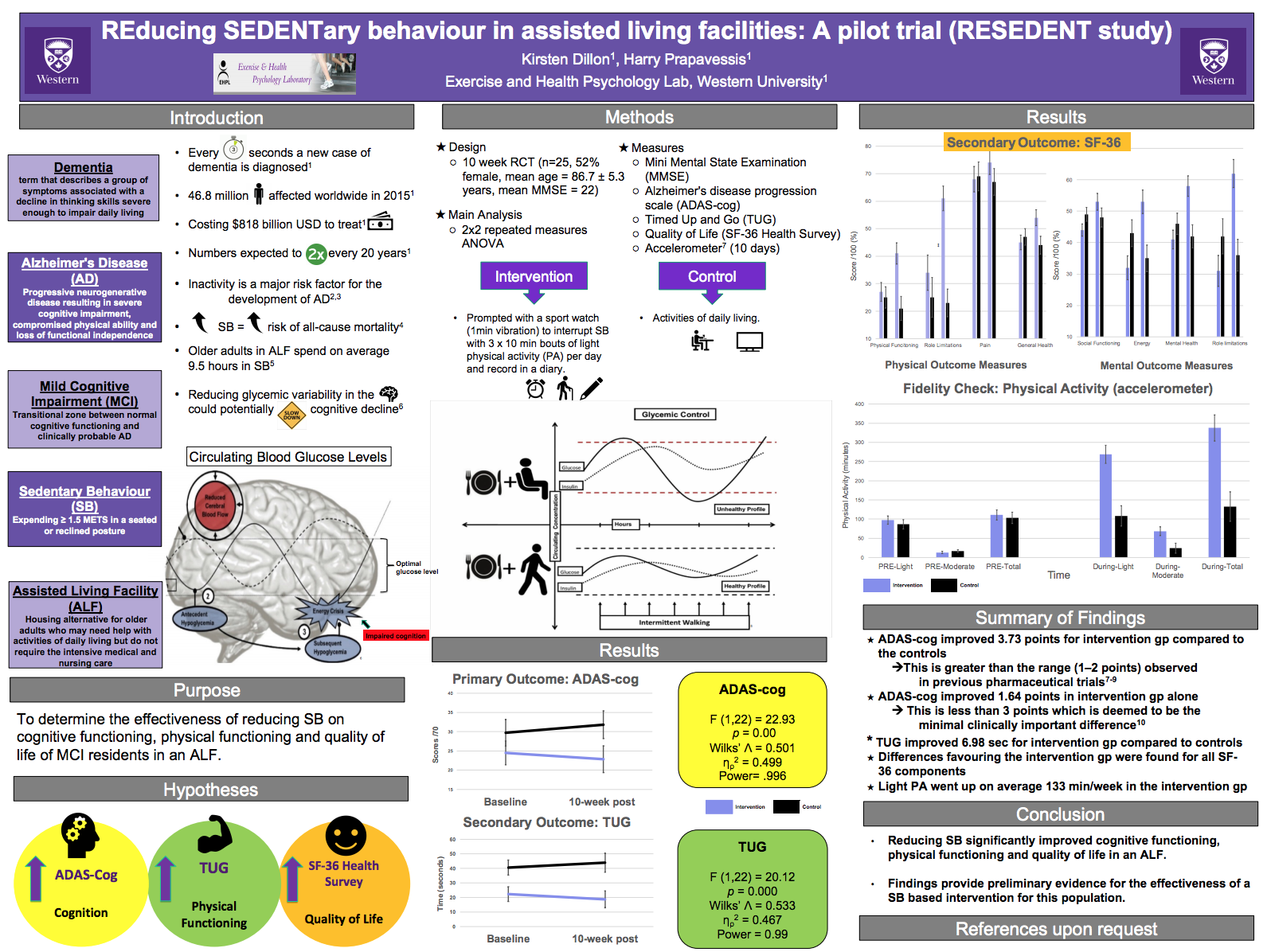
The RESEDENT study: REducing SEDENTary behaviour in senior living facilities: a Pilot trial
Dementia is an umbrella term used to describe a group of symptoms associated with memory loss severe enough to impact one’s abilities to perform activities of daily living. A new case of dementia is diagnosed every 3 seconds, with 46.8 million people worldwide affected in 2015 costing $US818 billion, and numbers expected to double every 20 years due to the rapid growth of the older adult population (Prince et al., 2015). In 2015, the World Health Organization (WHO) deemed dementia a public health priority; being the leading cause of dependence and disability worldwide (WHO, 2015). Currently, Alzheimer’s Disease (AD) is the most common form of dementia, making up approximately 60-80% of cases (Gaugler, James, Johnson, Scholz, & Weuve, 2017). Mild cognitive impairment (MCI) is generally used to refer to the transitional zone between normal cognitive functioning and clinically probable AD (Winblad et al., 2004).
Moderate-to-vigorous intensity exercise interventions show positive effects in attenuating cognitive decline in individuals already suffering with MCI or AD (Groot et al., 2016; McDermott et al., 2018). However, older adults are not partaking in sufficient amounts of physical activity (Colley et al., 2011) and instead, are spending up to 9.4 hours (65-80%) of their waking day sedentary (Harvey, Chastin, & Skelton, 2015). Sitting time has been established as a determinant of health and a modifiable risk factor for healthy aging (Owen et al., 2010). Sedentary behaviour (SB) is a distinct behaviour separate to that of merely being physically inactive. SB is defined as any waking behaviour characterized by an energy expenditure of less than or equal to 1.5 METs while in a sitting or reclining posture (Tremblay et al., 2017). Higher amounts of SB have been correlated with worse cognition and an increased risk of cognitive impairment regardless of physical activity time (Falck et al., 2016). That said, it is unknown what role SB plays in contributing to MCI and the progression of AD (Falck, Davis, & Liu-Ambrose, 2016). A recent hypothesis stated that we can potentially slow down cognitive decline by reducing glycemic variability in the brain, by replacing time sent in SB with light intensity PA (Wheeler et al., 2017).
The primary purpose of this pilot study was to investigate the effectiveness of reducing SB amongst mild to moderate cognitively impaired residents within in an assisted living facility and its impact on cognitive decline progression. A secondary purpose was to examine the interventions impact on residents’ physical functioning and quality of life. We used the Alzheimer’s Disease Assessment Scale-Cognitive (ADAS-cog) as our primary measure to assess cognitive function. The Time up and Go (TUG) and Short-Form 36 health survey (SF-36) were used to measure physical functioning and quality of life respectively.
We performed a 10-week single site randomized control trial. Twenty-five participants completed the study (52% female, mean age = 86.7 ± 5.3 years). The intervention group were prompted to interrupt their SB with three 10 min bouts of light physical activity throughout the day with a sport watch and record what exercise they did in a diary that was provided to them. The control group was just told to go about their usual activities of daily living; no diary was provided. As a fidelity check, an objective measure of physical activity was obtained using an Actical accelerometer (Philips Respironics, 920) for a 10-day period both pre and during intervention.
My primary objective was the total score on the ADAS-cog. The repeated measures ANOVA produced a significant time x group interaction effect for ADAS-cog scores F (1,22) = 22.93, p = 0.00, Wilks’ Λ = 0.501, ηρ2 = 0.499, power= .996. My secondary outcome was the TUG score. There was also a significant time x group F (1,22) = 20.12, p = 0.000, Wilks’ Λ = 0.533, ηρ2 = 0.467, power = 0.99. For quality of life, all measures improved for the intervention group and worsened for the control group. The fidelity check indicted that participants in the intervention group were in fact doing the exercise bouts. For more details see Kirsten's Thesis Poster.
The present pilot study explored the effectiveness of a SB based intervention and its impact on cognitive and physical functioning, as well as overall quality of life amongst older adults residing within an ALF. Findings provide preliminary evidence for the effectiveness of a SB based intervention for significantly improving cognition, physical functioning and quality of life. If future research can further establish positive effects from breaking up and reducing SB within ALF, polices can be implemented into these facilities to protect these older adults from further cognitive and physical functioning decline, preserving their independence.
Using motor imagery to maintain muscle mass following strength training
When physical movement is limited, for instance as the result of physical injury, lean muscle tissue and strength is lost. This is also the case with repeated sedentary behavior, such as extensive time sitting due to occupational constraints or in leisure time. One potential avenue to attenuate the loss of muscle strength and mass may be through the use of imagery.
Motor imagery is the mental rehearsal of a movement, in the absence of any physical movement. Imagery involves creating an experiences that mimics real experiences, and involves using a combination of different sensory modalities in the absence of actual perception. Research has shown that the use of imagery in immobilization-based studies can attenuate the loss in muscular size and strength when physical movement is not possible.
The aim of this study is to evaluate the effectiveness of a motor imagery intervention as a method for maintaining muscle mass and size, following a training program in untrained individuals. Eligible participants are enrolled in an 8-week muscle hypertrophy program for quadriceps using a leg press machine; after the 8 week program, participants are randomized to one of three groups. The maintenance group exercise with the leg press, but at a resistance equal to 40% of their maximum weight in order to maintain their quadriceps’ size and strength. The imagery group will sit on the leg press machine, but will be required to imagine completing a workout on the leg press machine without physically completing the movement. This will be verified through EMG feedback of the quadriceps. The control will use the bicep curl machine to target the bicep muscles.
This study has implications for guiding public health interventions, as well as offering efficacious strategies for maintaining muscle mass in individuals who may not have the time or means to properly exercise them.
For further information contact Alison (Ally) Divine adivine@uwo.ca
The effect of exercise on smokers' self-control
“Quitting smoking is easy; you just stop” most smokers would disagree with that statement. The truth is, quitting is hard. This is evident as 95% of smokers relapse within a year (CDCP, 2011). Quitting requires strong self-control (SC) (Muraven & Baumeister, 2000). SC, however, is a limited mental resource that is consumed when one exerts control over their thoughts, emotions, or behaviour.
Consuming too much SC depletes the resource leaving one susceptible to a breakdown in SC (Muraven & Baumeister, 2000). In fact, SC depletion increases lapse behaviour (Heckman, 2014). People trying to quit might relapse after undergoing depleting tasks, which can increase lapse behaviour in smokers and actually increases cravings in deprived smokers.
A single bout of moderately intense exercise alleviates cravings in abstinent smokers (Tart et al., 2010). Unfortunately, the mechanism by which exercise exerts its effect is not well understood. Previous findings have not supported any hypotheses. Therefore, future research should aim to better understand the acute effects of exercise. SC is a good candidate for further research due the nature of its relationship with smoking, lapse behaviour, and cravings. Abstinent smokers tend to relapse when experiencing cravings, which may be a consequence of depleting SC (Shiffman, 2000). Past research, however, has not looked explicitly at the relationship between SC strength and cravings. Therefore using the strength model of SC this study aims to examine whether exercise reduces cravings by replenishing SC which, in turn helps participants deal with cravings.
During the baseline assessment, male and female smokers will fill out questionnaires to obtain baseline measures of cravings and smoking habits. SC will be measured following the questionnaires using an isometric handgrip task. The handgrip task requires SC; as participants get tired they must resist the urge to quit and overcome fatigue to persist (Muraven & Baumeister, 2000). Participants will be randomly assigned to either the depletion only (DO) or the depletion + exercise (DE) group. They will be instructed to quit for the next 24h. In the second session, both groups will partake in a depleting thought suppression task. The DE group will then complete a moderate intensity exercise. This group is expected to have reduced cravings, and negative affect based on previous work (Tart et al., 2010). The DO group will sit passively and read a magazine, which will take as long as the exercise. Both groups will then provide SC strength measures through the isometric handgrip task and answer questionnaires to reassess their cravings. Current SC will be compared to the baseline measure. The main hypothesis will be supported if the DE group has decreased cravings and show less depletion then the DO group.Cravings are associated with a high risk of relapse (Shiffman et al. 1996). Understanding how exercise reduces cravings will not only enhance its credibility, but will also pave the road to creating interventions that maximize craving relief. Exercise is known to manage cravings effectively (Haasova et al., 2014) but it is less clear how effective it is if a person is dealing with stressors. This study will also add to the ecological validity of exercise as a craving intervention. People have to deal with daily stressors while they are trying to quit, this work will demonstrate whether exercise remains effective in reducing cravings after dealing with stressors. Furthermore, this line of research offers a healthy alternative to those not interesting in pharmacological interventions. Exercising provides many health benefits and reduces the risk of mortality (Woodcock, Franco, Orsini, & Roberts, 2011). Therefore using exercise to reduce cravings can both help those struggling with their cravings while simultaneously improving ones health.
For further information contact Steven Guirguis sguirgu4@uwo.ca
Using a HAPA based intervention to reduce sedentary time in university students
Sedentary behaviour is strongly associated with a broad spectrum of chronic diseases, ranging from heart disease, to diabetes, to hypertension – all independent from levels of moderate-vigorous physical activity. Sitting, the most common form of sedentary behaviour, is prevalent in nearly all aspects of daily living, including: occupation, transportation, meals, screen time, etc. Given the diversity between lifestyles, and consequently sitting profiles, some populations are much more sedentary than others. University students are an example of a population at high risk for excessive sedentary behavior, with time spent seated in class and while studying (i.e. Occupational sitting) comprising a significant portion of their sitting profile. Recent research has shown that simply taking more frequent, and longer breaks from sitting (e.g. standing, walking, etc.) are an effective way to reduce the health risk associated with excessive sedentary behavior. The excessive occupational sedentary behavior that full-time university students are subject to makes them an ideal population for behavioral intervention.
There is often a disconnect between the intentions that a person has to perform a behavior, and the behavior itself; this is sometimes referred to as the “intention-behavior gap”. The Health Action Process Approach model, or HAPA, is a behavioral model that seeks to bridge the intention-behavior gap through the use of Action Planning and Coping Strategies. The model is centred on self-efficacy, or one’s belief in oneself to execute behaviors necessary to perform certain behaviors (Bandura, 1977). Simply put, the model uses Action Planning and Coping to bolster the self-efficacy required by an individual to successfully perform a behavior.
The aim of this study is to utilize the HAPA model in order to target, and measure the reduction in occupational sedentary time in full-time University students. Eligible participants are full-time Western University students over 18 years of age in good physical and mental health. The study is 6 weeks in length, with a 2 week follow-up. Eligible consenting participants will fill out both a 7 day food recall questionnaire, as well as the modified SIT-Q 7d Questionnaire – a questionnaire designed to reflect both domain specific sedentary time and frequency/duration of breaks taken from sitting. Participants will then be randomized to either nutrition or sedentary behavior counseling. The counseling sessions will focus on creating specific action plans and coping strategies for the randomized behavior. After the first meeting, participants will receive weekly emails containing the SIT-Q 7d Questionnaire. Three weeks after the initial meeting, participants will return to the lab for a second counseling session, as well as filling out the dietary recall questionnaire and modified SIT-Q 7d. Weekly emails will be resume for the remaining three weeks of the study. A follow up modified SIT-Q 7d will be sent 2 weeks after the study period has ended.
Primary measures will include total occupational sitting time, as well as frequency and duration of breaks taken from occupational sitting; compared at all three time points: baseline, 3 weeks and 6 weeks.
Reducing excessive sedentary behavior is vital to reducing the risk for chronic diseases. University students are subject to excessive occupational sedentary behavior as a product of their education. The results of this study will help to build and guide future interventions for reducing the amount of occupational sedentary behavior that university students, and other populations, engage in.
For further information contact Yoah Wuyou Sui wsui3@uwo.caGetting Physical on Cigarettes: Smoking Cessation and Relapse Prevention for Women
Lung cancer is the leading cause of cancer death in Canadian women, and with an estimated 10,900 new cases, lung cancer is second behind breast cancer as the leading type of cancer in women (Canadian Cancer Statistics, 2007). It is recognized in all Canadian health strategy documents that stopping smoking at any age is associated with clear health benefits (Health Canada, 2007), including a decreased risk of lung cancer. Unfortunately, the nicotine found within cigarettes is highly addictive (Hirschhorn, 2008), making it difficult for many smokers who wish to quit to successfully abstain.
Adding exercise to cognitive behaviour therapy (CBT) has been shown to aid smoking cessation and lessen some of the negative consequences of withdrawal symptoms (Marcus et al., 1999; Ussher, 2005). Recently, Prapavessis and colleagues (2007) demonstrated that their 12-week program, consisting of supervised vigorous intensity exercise as an adjunct to nicotine replacement therapy (NRT), facilitates smoking cessation, improves physical fitness, and delays weight gain in women smokers. However, a smoking relapse effect was shown post-intervention, illustrating a trend where, as abstinence decreased, physical fitness showed a corresponding decrease and an increase in weight (also see, Marcus et al.). These results suggest that exercise needs to be maintained if it is to be an effective aid to smoking cessation.
In practice, long-term supervised and structured vigorous exercise regimes are beyond the scope of smoking cessation services. Therefore, it is important to determine whether an exercise intervention program can be developed to maintain weight and physical fitness after program termination, and thus prevent (or reduce) smoking relapse. Teaching smokers the necessary self-regulatory skills needed to abstain from smoking and adhere to exercise independently may be a promising avenue through which to ensure lasting health behaviour changes.
The Getting Physical on Cigarettes program will begin in January 2010. The main purpose of this project is to examine whether an inexpensive, home-based lifestyle exercise maintenance intervention can demonstrate sustained health benefits in terms of weight gain and physical fitness benefits following an exercise and NRT-aided smoking cessation program. In addition, this trial seeks to examine previously unexplored topics of interest in the smoking abstinence literature; specifically, we are interested in whether the nicotine metabolite ratio (3-HC/Cotinine: Schnoll et al., 2009) is a useful biomarker for determining cessation success in relation to exercise and NRT treatment, and whether the interactive effects of exercise and smoking cessation improve vascular health and lung function.
Four hundred and twenty adult female smokers will follow a structured and supervised 14 week exercise-aided smoking cessation program, with the 10 week NRT program beginning at week 4. Participants will be randomized into one of four conditions: a) Exercise Maintenance; b) Exercise Maintenance + Relapse Prevention Booklets; c) Relapse Prevention Booklets + Contact; and d) Contact Control. Starting at week 8, women in the Exercise Maintenance conditions will engage in group mediated cognitive behavioural therapy (GMCB) related to maintaining exercise in their home environment, while women in the Contact conditions will partake in group mediated discussions related to other health issues. The “Forever Free” series (Brandon, Collins, Juliano, & Lazev, 2000) will be distributed to participants in the Relapse Prevention Booklets conditions; however, all groups will receive the same amount of supervised exercise sessions and NRT prior to randomization. Following the termination of the 14 week intervention all participants will be contacted by a trained facilitator, who will deliver 15 minute biweekly (for the first month), monthly (for the next 2 months), and then bimonthly (for last 8 months) intervention strategies over the phone to continue to counsel the women according to her particular group-mediated condition.
Primary end points (i.e., smoking abstinence) will be assessed weekly throughout the 14 week program and through follow-ups at 3 and 12 months. Secondary end points (i.e., fitness, vascular health [e.g., endothelial function, carotid plaque volume], lung function, weight and self-regulatory cognitions) will be assessed at baseline and at week 14 as well as at 3 and 12 months. Accelerometers (ACTICALÒ) will be used to obtain an objective measure of physical activity at baseline, week 15 (1 week after the 14 week intervention) and at 3 and 12 months.
The Getting Physical on Cigarettes trial will not only contribute to a better understanding of the role exercise plays as an aid to smoking cessation, but will also explore a means of increasing the cost-effectiveness of long-term smoking cessation programs. The findings resulting from this trial may have important implications for improving the quality of life among individuals who wish to stop smoking, which would, in turn, have a significant impact on the cost of health care to the Canadian public.
This 3-year project is supported by the Canadian Cancer Society Research Institute (Grant # 019876).
To read about the preliminary results of the trial click here
For further information about the trial contact Lyndsay Fitzgeorge: lfitzgeo@uwo.ca
Prehabilitation for Knee Replacement
Osteoarthritis is one of the most prevalent conditions affecting adults worldwide, and the symptoms are generally worse in weight-bearing joints like the hips and knees. For those with end-stage symptoms, such as severe stiffness, pain, and reduced mobility, joint replacement surgery (or arthroplasty) is often the only option. Patients with greater muscle strength tend to have more positive outcomes after surgery, so it has been suggested that exercise programs for improving strength before surgery may have some benefit.
The Prehabilitation for Knee Replacement Study is an exercise program designed to improve fitness and strength in adults aged 45-64 who are scheduled for knee replacement surgery. Participants exercise 3 times per week for 12 weeks leading up to their surgery date, and are monitored for strength gains every 2 weeks. Following surgery, there are follow-ups at 3, 12, and 24 weeks to assess strength, range of motion, pain, and psychological variables (ex: self-efficacy and quality of life).
For further information about this trial contact Carly Mckay cmckay22@uwo.ca
Adolescent Fitness Assessment Program
There has been a dramatic increase in the prevalence of overweight and obese children in all regions of Canada (Willms et al., 2003). This is disconcerting because this preventative condition is strongly associated with the risk of future disease, including adult obesity, insulin resistance (IR), type II diabetes, cardiovascular problems and psychosocial distress. This trend is a driving factor to develop effective strategies for assessment and intervention.
Aerobic fitness is the ability of the heart and lungs to deliver oxygen to working muscles, in addition to the ability of those tissues to use that oxygen to produce energy. It is measured as peak VO2 (mL/kg min), and is evaluated using a maximal incremental exercise protocol on a treadmill. Aerobic fitness is a strong indicator of physical activity and also correlates with IR and the aforementioned diseases. Aerobic fitness values also appear to yield inconsistent results in youth, particularly obese youth (Korsten-Reck et al., 2006).
The purpose of the Adolescent Fitness Assessment Program is to examine changes in fitness tests in overweight and obese youth over a two week period after participants watch a short, educational film. Participants will be asked to complete two aerobic fitness tests and questionnaires over a two week period at the Exercise and Health Psychology Lab, University of Western Ontario.
For further information about this trial contact Stefanie De Jesus sdejesus@uwo.ca
Exercise, Metformin & Obesity Study: Reduction of Adolescent Risk Factors for Type-2 Diabetes and Diabetes-related Cardiovascular Disease
Childhood obesity is a serious health concern associated with increased risk of Type 2 Diabetes. Given that one of the most frequently cited causes of the current childhood obesity epidemic is the high rate of physical inactivity in youth today, it is essential to develop and implement physical activity interventions to help obese children make long-term health behaviour changes.
The purpose of this randomized controlled trial is to help obese adolescents develop the self-regulatory skills needed to initiate and maintain regular physical activity (PA). Sixty obese adolescents (age 10-16) and their parents will be recruited for this study that will last for two years. Once the adolescent and their parent(s) are deemed eligible, they will be randomized into the following four treatment groups: moderate exercise (ME) + metformin, ME + placebo, vigorous exercise (VE) + metformin, and VE + placebo. All participants will come to the Exercise and Health Psychology Lab (EHPL) to exercise for 1 hour, 3 times a week for the first 12 weeks of the program. Both groups will participate in a group-mediated cognitive-behavioural intervention that will target constructs of Bandura’s (1986) Social Cognitive Theory (e.g., goal-setting) thought to facilitate long-term behavioural changes. Participants will meet with a dietician, social worker and pediatrician on a monthly basis for the first year of the study, and every three months during the second year of the study.
Throughout the two-year study participants will complete body composition (DXA) measures, cardio-respiratory and strength fitness assessments, questionnaires assessing their quality of life, self-efficacy, outcome expectations, and both subjective (self-report) and objective measures of physical activity. Physical and psychosocial variables will be assessed at baseline, 6-weeks, 12-weeks, and 1, 3 and 6, 12, 18 and 24-months follow-up.
For further information about this trial contact Justine Wilson awils29@uwo.ca
Examining the acute effects of a scenic nature video on mood following a 30-minute moderate intensity run
The importance of exposure to the natural environment on enjoyment of physical activity has become a popular topic within exercise psychology. Previous research has demonstrated that contact with the natural environment has a positive impact on mood through decreases in stress and mental fatigue (Health Council of The Netherlands, 2004).
This positive affective response has been has associated with the restorative effect of nature itself. Recent research has demonstrated that exposure to nature has a higher restorative effect on individuals than remaining indoors, or have outdoor exposure to the built environment (Van den Berg, A.E., Hartig, T., &Staats, H., 2007). However, exposure to the natural environment may not be practical for everyone in an increasingly populated world. Cities and urban centers are growing larger, with upwards of 75% of the world’s population living in densely populated areas (Habitat, 2001). Thus, it is important for health researchers to examine the potential environmental exposure opportunities for individuals living in urban areas.
Recent research has explored visual representations of the natural environment, such as videos or photographs, on individual’s mood. In an exercise specific context, Van den Berg and colleagues (2007) displayed multiple photographs of a natural setting while fatigued participants walked indoors on a treadmill for 20 minutes. This experimental condition was compared to two control conditions, one consisted of a group of individuals who walked while being presented with photographs of the city, and the other was a no stimulus control. Results demonstrate that individuals who participated in the nature simulation walk felt less fatigued and had more energy than either control condition. These results provide initial evidence that individuals exposed to depictions of nature can have similar positive changes in affect as those who exercise outdoors.
This study extended these findings to a group of regular runners. Specifically, the study examined the effects of jogging for 30-minutes while watching a nature video on participant’s mood. This nature video consisted of a simulated run through a natural environment. Mood changes among these individuals were compared to those among three conditions: (a) watching a video of parking lot activity, (b) watching neutral television program, and (c) not watching a video at all. Individual’s mood was measured before, during, and after exercise. Exercise and video enjoyment were also assessed. It was hypothesized that individuals in the nature condition would experience more positive changes in mood than the other three conditions. It was also hypothesized that they would report higher levels of enjoyment of the activity and the video.
While affect was found to positively increase in each of the four conditions, repeated measures MANOVAs revealed no significant differences between the conditions. However, enjoyment of the run was positively correlated with affective response. It was concluded that a nature simulation video does not appear to influence affect differently than other visual stimuli during a 30-minute run in a sample of regular runners.
Further research would do well to investigate the effects of a similar nature simulation intervention among individuals who are not regular exercisers and/or regular runners. It is expected that individuals who are not regular runners would be more likely to benefit from a nature simulation video while running because they are less likely to inherently enjoy the run itself. Using a sample of non-exercisers or non-runners would likely result in higher variability among affective response scores in the different conditions.
Future research should also explore the use of nature simulation videos on individuals as they run at a set intensity or pace. The current study allowed participants to set the treadmill speed to what they felt was a moderate intensity and adjust it accordingly throughout the run. It would be interesting to explore affective responses to the video intervention when participants were forced to run at a set pace or a specific intensity.
Pre and Postnatal Smoking Cessation Studies
In recent years, exercise has gained increased attention in terms of its effectiveness in attenuating smoking desire, withdraw symptoms and cravings that may help cope with smoking abstinence (Ussher, 2007). Although evidence exists that exercise aids smoking cessation among the general population, this evidence has not been extended specifically to pre and postnatal women. This is unfortunate because exercise may be a highly successful strategy because:
-
- Pregnant and postnatal women are unable to use traditional pharmaceutical smoking cessation therapies
- Postnatal women are motivated to exercise in order to return to their pre pregnancy weight and shape
- Pregnant and postnatal women may be concerned about weight gain or mood related changes associated with smoking cessation. Exercise has been demonstrated to have a positive impact on both these concerns.
However, quitting smoking and engaging in regular exercise are both extremely challenging health behaviours. Despite pregnant and postnatal women being highly motivated to quit smoking and exercise regularly, successful adherence to both behaviours is difficult. Our goal is to help pregnant and postnatal women achieve these two health benefits. How?
-
- Free professional assistance helping participants adopt a healthy lifestyle including regular physical activity and becoming/remaining smoke free. Successful adherence to the program may result in many short-term and long-term health benefits for both the mother and child.
- Free access to a state of the art exercise facility
- Free exercise training program
- Free cognitive behavioural counseling sessions that will help participants quit smoking or remain smoke-free.
- Free childcare while attending the program
Who are we looking to recruit?
Pregnant and postnatal women (within 52 weeks of giving birth) in the London area who either:
- Have quit smoking and want help remaining smoke-free
- Are currently smoking and want help quitting
What does the study consist of?
There are 2 parts:
- A one-time treadmill walking session
- An 8-week intervention, where participants come into our private exercise facility 2x/week. Each session will include exercising for 30 – 45 minutes and cognitive behavioural training sessions targeting at behavior change (e.g., increasing physical activity into your lifestyle and smoking cessation counseling).
**Note participants will complete the first part and then be asked if they want to join the 8-week program. There is no commitment to complete the 8-week program if they complete part 1.
If you are interested in this study and would like to register, please select the study arm that describes you:
Prenatal Smoking Cessation – “I am pregnant and want to quit smoking”
(link: http://ehplwebq.vm.its.uwo.ca/survey/elig_preg_sc)_
Postnatal Smoking Cessation – “I am postnatal and want to quit smoking”
(link: http://ehplwebq.vm.its.uwo.ca/survey/elig_pn_sc)
Prenatal Smoking Relapse Prevention – “I am pregnant and want help remaining smoke-free”
(link: http://ehplwebq.vm.its.uwo.ca/survey/elig_preg_q)
Postnatal Smoking Relapse Prevention – “I am postnatal and want help remaining smoke-free”
(link: http://ehplwebq.vm.its.uwo.ca/survey/elig_pn_q)
The effect of a media literacy intervention on body dissatisfaction
Exercise videos have been promoted as motivational exercise tools (Markula, 1995). While exercise videos may initially motivate consumers to achieve this figure by using the video, the instructor is usually found to be physically dissimilar, and intimidating (Fleming & Martin Ginis, 2004; Markula; Maguire & Mansfield, 1998). Media literacy – fostering critical thinking of societal ideals - has demonstrated to be an effective tool to counteract the negative effect that media images have on women (Posavac et al., 2001).
The purpose of this study was to compare the effect of Posavac’s (2001) media literacy intervention to an attention control using an exercise video. It was hypothesized that exposure to the intervention would lead to an increase in body satisfaction from baseline after watching and exercising to an exercise video.
The assessment was a crossover experimental design. Non-exercising female (M age = 23.54; SD = 7) participants with body image concerns (n = 24) were randomized into either a media literacy or an attention control treatment group. Participants then watched and worked-out to an exercise video for five and 20 minutes, respectively. Following each video condition, participants completed body image subscale measures of Appearance Evaluation and Body Area Satisfaction (Brown, Cash, & Mikulka, 1990).
Results (see Figure 1 and 2 below) reveal significant interaction effects on both body satisfaction measures where the control group demonstrated a significant increase in body satisfaction from baseline to watching. The exercise condition did not show significant interactions, eluding to differences between passive and active behaviour on one’s body image perceptions. These findings can be attributed to self-enhancement (Shrauger, 1975) and appearance investment (Cash, 2003) theories.
For further information about this trial, please contact Joy Elkayam jelkayam@uwo.ca
Figure 1
p < .01, n² = .27
Figure 2

p = .05, n² = .19
The Effects of Acute Exercise on Tobacco Cravings and Withdrawal Symptoms in Pregnant Women
One purpose of the proposed study is to examine the effect of 20 minutes of moderate intensity exercise and 20 minutes of light intensity exercise on desire to smoke and withdrawal symptoms in pregnant women. Another purpose is to examine possible biological mechanisms (i.e., cortisol and dopamine) which might explain how exercise works in reducing both the desire to smoke and withdrawal symptoms. Sixty inactive pregnant smokers between the age of 20 and 40 will be recruited and then randomly assigned to one of three conditions: (i) moderate exercise (n= 20); (ii) mild exercise (n = 20); and (iii) passive control (n =20). All participants will be asked to abstain from smoking for approximately 18 hours. Tobacco craving and withdrawal symptoms will be completed at baseline, midpoint exercise (10 minutes), immediately following exercise (20 minutes), and at 10, 20, and 30 minutes post exercise.
This study will provide valuable insight into the level of intensity of exercise needed to reduce craving and withdrawal symptoms for pregnant women. In practice, doing mild to moderate instead of vigorous levels of exercise to obtain craving and withdrawal reductions is easier for most inactive people. Furthermore, current physical activity recommendations encourage short, intermittent and daily bouts of mild-to-moderate intensity exercise. This study also will provide valuable insight into the mechanism(s) by which exercise may contribute to greater abstinence. Understanding the mechanisms (i.e., cortisol) is vital as it offers precise guidance and understanding for both the health professional and quitter. Furthermore, this trial will serve as an excellent platform for conducting other types of acute smoking trials in pregnant women. For instance, there is limited evidence demonstrating the impact exercise has on urges to smoke during smoking cues and on ad libitum smoking. Second, a solid foundation can be laid for eventually conducting large RCTs involving exercise and smoking cessation in pregnant and postpartum women.
For further information about this trial, please contact Therese Harper tharper2@uwo.ca
Initiating and Maintaining Exercise Behaviour in First- and Second-Degree Relatives of Colon Cancer: A Matter of Self-Regulation
In 2007, an estimated 20,800 Canadians will be diagnosed with colon cancer and 8,700 will die of it making colon cancer the second leading cause of death from cancer (Canadian Cancer Society, 2007). Given the protective benefits of exercise for colon cancer, there is a need to develop and test novel, innovative and inexpensive ways to increase the likelihood that people, and in particular those with an elevated risk (first- and second-degree relatives) will adopt healthy exercise patterns.
This Social Science and Humanities Research Council of Canada (SSHRC) funded research study is intended to examine the effectiveness of an intervention strategy grounded in Self-Regulation Theory that seeks to modify (enhance) exercise behaviour in first- and second-degree relatives of colon cancer patients. The exercise interventions strategies are intended to effectively motivate activity change as a first step (Phase I), and then facilitate the initiation, adoption (Phase II), and maintenance of exercise (Phase III). Using an aggressive advertising campaign and having access to the Ontario Colon Cancer Family Registry we plan to initially recruit 200 colon cancer relatives to ensure that 130 participants complete the trial.
Phase I: Initiating Physical Activity Behaviour:
The primary purpose of Phase I is to examine whether colon cancer prevention information can motivate inactive, first- and second-degree relatives of colon cancer patients to consider exercising using Protection Motivation Theory (PMT). While a secondary purpose of the study is to examine whether an individual’s belief about exercise and colon cancer can be changed.
Thus far 98 first- and second-degree relatives of colon cancer patients have been randomly assigned to either an intervention (n=52) or an attention control group (n= 46). At baseline, participants completed demographic information, the Stage of Exercise Readiness Questionnaire and the Beliefs towards Exercise and Colon Cancer Questionnaire. Beliefs towards Exercise and Colon Cancer Questionnaire, contains four items for each of the PMT constructs (vulnerability, severity, self-efficacy and response efficacy) as well as three intention items. The items are rated on a seven-point Likert scale (1= strongly disagree to 7= strongly agree). A week following baseline measures, participants returned to the lab to view a DVD. The intervention groups DVD, presented factual information by leading Oncologists and Kinesiologists on exercise and colon cancer and was designed to manipulate the four PMT constructs. The attention controls DVD presented general nutrition information as well as discussed nutrition’s relationship to cancer. Following the DVD, participants again complete the Beliefs towards Exercise and Colon Cancer Questionnaire.
To analyze the results a 2 (group) x 2 (time) repeated measures ANOVA was conducted to examine the group by time effects for the PMT constructs. Additionally, regression analysis was conducted to explore which PMT constructs predicted intention Pre- and Post-DVD. See the preliminary results below.

Figure 1. Vulnerability scores pre-DVD and post-DVD.

Figure 2. Severity scores pre-DVD and post-DVD.

Figure 3. Self-efficacy scores pre-DVD and post-DVD.

Figure 4. Response efficacy pre-DVD and post-DVD.

Figure 5. Intention scores pre-DVD and post-DVD.
Table 1. Predicting Intention Pre-DVD
|
|
b |
t |
R |
R2 |
|
|
|
|
.49** |
.21** |
|
Severity |
.18* |
2.07* |
|
|
|
Self-Efficacy |
.27** |
2.99** |
|
|
|
Response Efficacy |
.28** |
3.00** |
|
|
**p <0.001; *p <0.05
Table 2. Predicting Intention Post-DVD
|
|
b |
t |
R |
R2 |
|
|
|
|
.75** |
.55** |
|
Vulnerability |
.04 |
.48 |
|
|
|
Severity |
.20* |
2.60* |
|
|
|
Self-Efficacy |
.54** |
7.22** |
|
|
|
Response Efficacy |
.23* |
2.78* |
|
|
**p <0.001; *p <0.05
Take Home Message: The results demonstrate that a single exposure media intervention grounded in PMT can change individuals’ exercise and colon cancer beliefs as well as their exercise intentions.
For further information about this trial, please contact Erin McGowan emcgowa@uwo.ca
Phase II: Adoption and Maintenance of Physical Activity Behaviour in a 12-week Structured Exercise Program
Purpose:
The purpose of Phase II is three-fold: (1) to test a self-efficacy intervention (both task and self-regulatory) in influencing adherence to a 12-week structured exercise program, (2) to examine self-efficacy (i.e., both task and self-regulatory) in predicting exercise adherence, and (3) to explore the temporal patterns of self-efficacy in a 12-week structured exercise program.
Methods:
One hundred and forty first- and second-degree relatives of colon cancer patients (M=45.5 years, ±9.0; 88.6% first-degree relatives; 70.7% female) were enrolled in a 12-week exercise program, and were randomized to either self-efficacy intervention (INT) or to an attention control (AC) condition. At the start of the exercise program participants were given exercise guidelines to follow. Weekly the INT group and the AC group took part in classroom sessions that lasted between 20 to 45 minutes. The intervention material focused on promoting scheduling, barrier, goal setting and relapse prevention efficacy, while the control material focused on nutrition information. Adherence to the exercise program was assessed through objective measures of frequency, duration and intensity of exercise, as well as through attrition rates, while self-efficacy was assessed at baseline, weeks 4, 8, and 12. A dropout was classified as someone who did not exercise for 6 consecutive weeks.
Results:
Testing Self-Efficacy Intervention:
Separate two (group) by three (time- 4, 8, 12) repeated measures ANOVAs showed that there was a significant interaction effect for duration (p = .001, η2= 0.07) (see Figure1), but not for intensity (p =.24, η2= 0.02) and frequency (p = 0.17, η2= 0.03). Planned comparisons test for duration showed that early in the exercise program (i.e., 0 to 4 weeks) the INT group exercised significantly longer F (1, 138) = 1.98, p= .02 than their AC counterpart. Finally, a chi-square analysis revealed that dropouts between groups were different at week 4 χ2 (1, N = 154) = 2.88, p = .08; week 8 χ2 (1, N = 154) = 5.54, p = .02; and week 12 χ2 (1, N = 154) = 2.50, p = .08. Specifically, 87.5% and 95.1%; 68.1% and 84.1%; and 65.3% and 76.8% of the AC and INT group was retained at week 4, 8 and 12 respectively (see Figure 2).
Figure 1. Exercise duration across time points for the INT and AC groups
Figure 2. Drop-out Behaviour across time points for the INT and AC groups

Predicting Exercise Adherence:
Proxy self-efficacy variables that showed a relationship to exercise adherence were entered into a regression (e.g., baseline self-efficacy to exercise adherence at week 4). The best predictor of exercise frequency at week 8 was scheduling efficacy, while at week 12 the best predictors were scheduling and task efficacy, explaining 16.0% and 16.2% of the response variance, respectively. For exercise duration at week 8 and 12, the best predictors were task and scheduling efficacy, explaining 11.5% and 12.5% of the response variance, respectively. The best predictors of exercise intensity at week 8 were task and scheduling efficacy, while at week 12 the best predictor was task efficacy, explaining 14.1% and 9.7% of the response variance, respectively.
Temporal Patterns of Self-Efficacy:
Task and barrier efficacy increased significantly during the 12-week exercise program (p < .001; η2 = .40; p < .001; η2 = .24, respectively), while scheduling efficacy decreased (p = .10; η2 = .05). Both goal-setting and relapse prevention efficacy remained stable throughout the exercise program (p = .90; η2 = .00; p = .38; η2 = .02, respectively). See Figure 3.
Figure 3. Temporal Patterns for Self-Efficacy 
Conclusion:
An intervention grounded in self-efficacy theory is effective in assisting relatives of colorectal cancer adopt and maintain a 12-week exercise program. Self-efficacious beliefs are associated with objective dose measures of adherence from week 8 onwards in a 12-week exercise program. The self-efficacious beliefs examined have different temporal patterns.
For further information about this trial, please contact Erin McGowan emcgowa@uwo.ca
Phase III: Adoption and Maintenance of Physical Activity Behaviour in a 9 Month Home-Based Exercise Program
Background:
Few intervention strategies aimed at changing physical activity and exercise behavior have produced long-term behavior change (Rothman, 2000). This demonstrates that behavior change and maintenance are complex issues that require both self-regulation and self-efficacy. Self-regulation represents the ability to change oneself and exert control over one’s inner processes (Baumeister & Vohs, 2004), while self-efficacy reflects “beliefs in one’s capabilities to organize and execute the course of action required to produce given attainments” (Bandura, 1997).
Purpose:
The objectives of the present study were to (a) examine the effect of a self-efficacy (i.e., task and self-regulatory) intervention on physical activity in relatives of colon cancer patients undertaking a 9-month home-based physical activity program, (b) examine the effect of a self-efficacy intervention on task, barrier, scheduling, goal setting and relapse prevention efficacy in relatives of colon cancer patients undertaking a 9-month home-based physical activity program, and (c) examine the self-efficacy and self-regulation model in predicting objective physical activity behavior.
Methods:
Following a 12-week structured exercise program, relatives of colon cancer patients (N =107; M=45.7 years, ± 8.7; 91.0% first-degree relatives; 67.3% female) participated in a 9-month home based physical activity program. Participants remained in the same randomized condition: self-efficacy (intervention) or nutrition (attention control). The intervention group received monthly emails that focused on self-efficacy information (e.g., task, scheduling, barrier, relapse prevention), while the attention control group received nutrition information. Physical activity (i.e., energy expenditure; EE = daily kcals/min/kg) was objectively assessed using Actical® accelerometers at 1 week following the exercise program, and at 1, 3, 6, and 9 months. Self-efficacy was assessed at all these time points except month 1.
Results:
Effect of a Self-Efficacy Intervention on EE:
A factorial repeated measure ANOVA revealed a significant time effect for EE, F(1, 56) = 3.43, p < .05; η2 = .20. Specifically, EE systematically declined over the 9 months. No interaction effect F (1, 56) = .41, p =.80; η2 = .03 was found. However, the intervention group (M = 755.26, SE= 44.19; 772.59, SE = 71.27; 792.23, SE = 62.17; 686.15, SE= 40.02; and 664.60, SE= 50.38) had higher EE at all time points compared to the attention control group (M = 721.84, SE= 35.74; 704.85, SE= 41.95; 667.26, SE= 42.95; 618.28, SE=35.23; and 633.68 SE=41.50, respectively). See Figure 1.
Figure 1. EE across time points for the INT and AC groups 
Effect of a Self-Efficacy Intervention on Self-Efficacy Levels:
A factorial repeated measure ANOVA revealed significant main effects for time for task (η2 = .18), scheduling, (η2 = .28), goal setting, (η2 = .39), and relapse, (η2 = .37), such that all self-efficacy measures decreased across time. A significant group by time interaction effect was present for barrier, (η2 = .13). Whereas barrier efficacy scores decreased across all time points in the attention control condition, barrier efficacy scores initially declined, followed by an increase and subsequent decrease across assessment points in the intervention condition (see Figure 2).
Figure 2. Barrier efficacy across time points for the INT and AC groups 
Self-Efficacy and Self-Regulation Model in Predicting Objective Physical Activity Behavior:
Proxy self-efficacy variables that showed a relationship to EE were entered into a regression (i.e., week 1 self-efficacy predicting PA at month 1). Results revealed that week 1 self-efficacy variables predicted EE at month 6, and month 3 self-efficacy variables predicted EE at month 6, accounting for 11.1% and 8.8% of the response variance respectively.
Conclusion:
An intervention grounded in both task and self-regulation efficacy was modest in assisting relatives of colon cancer patients adopt and maintain their physical activity in a 9 month home-based physical activity program. With the exception of barrier efficacy, the intervention was unsuccessful in preventing decreases in self-efficacious beliefs in a 9 month home-based exercise program. Self-efficacious beliefs are associated with objective measures of physical activity over a 9-month home-based program.
For further information about this trial, please contact Erin McGowan emcgowa@uwo.ca
Motivating Pregnant Women to Exercise
Despite the confirmed health benefits of exercise during pregnancy, many expectant mothers are not sufficiently active. The present research used a Protection Motivation Theory (PMT) framework to examine whether information about the role of exercise in preventing several maternal-fetal diseases served as a meaningful source of exercise motivation. Participants were 208 pregnant women randomly assigned into one of three treatment conditions: PMT present, attention control, and non-contact control. Baseline demographic and self-reported exercise behavior was collected prior to treatment. Women in the PMT present group read a brochure about the benefits of exercise during pregnancy which incorporated the four major components of PMT; perceived vulnerability (PV), perceived severity (PS), response efficacy (RE) and self-efficacy (SE) as well as exercise tips and suggestions. Participants in the attention-control condition read a brochure about diet and pregnancy. Following treatment, all participants completed questionnaires which assessed their beliefs towards maternal-fetal disease and exercise in addition to goal intention (GI) and implementation intention (IMI) scales. One week later, a follow-up measure of self-reported exercise behavior was once again collected. Only women who were under 30 weeks pregnant were used in subsequent analyses (n = 105). Separate ANOVAs followed by planned comparisons were conducted for the four PMT constructs and two intention constructs. Results showed that compared to the two control groups, participants assigned to the PMT present group reported significantly higher PS (η2= .11, p = .002), RE (η2= .28, p = .000), SE (η2=.11, p = .003), and GI (η2= .12, p = .002,). No significant differences were found for IMI (η2=.02, p = .33). For exercise behavior, a repeated measures ANOVA showed a significant interaction effect (η2 = .41, p = .001), where only the PMT intervention lead to increases in follow-up exercise behaviour (see Figure 1 below). Regression analyses revealed that PS, RE & SE accounted for 51% of the variance in GI, GI accounted for 12% of the variance in IMI, and IMI accounted for 12% of the variance in follow-up exercise behavior. Overall, the present research demonstrates that a single exposure to information about the role of exercise in preventing maternal-fetal disease grounded in a PMT framework can influence pregnant women’s beliefs, motivation and initial behavior.
For further information about this study, please contact Anca Gaston at ancagaston@gmail.com
Figure 1. Mean and SE scores in exercise behavior between treatment groups across time.

Validation of the ACTIHEART™
This study looks to validate a novel objective measurement tool, called the Actiheart™ which simultaneously collects real time heart rate and movement counts for the measurement of physical activity energy expenditure (PAEE). To date, the combination of heart rate and movement counts together provide a more accurate measure of PAEE than either method alone. The Actiheart™ has previously been assessed as an accurate measure of PAEE in both an adult and child population. The device was assessed for structured treadmill walking and running exercise and simulated real life activities such as washing windows, folding laundry and shovelling dirt. Unfortunately, the Actiheart™ remains to be validated as an accurate measure of PAEE for free-living activity. Without a precise quantification of PAEE from these types of activities, perceptions regarding what type of lifestyle (sedentary, moderately active, or active) Canadians lead may be skewed.
The primary purpose of the current study is to demonstrate the Acitheart™ as an accurate measure of PAEE in an adolescent population for both a structured activity, as well as for the volitional day-to-day activities adolescents partake in during their daily lives. Using a two part design, PAEE predictions derived using the Actiheart™ will be compared to criterion measures of PAEE via indirect calorimetry (Part I) and doubly labelled water (DLW) (Part II) for lab-based exercise and free-living activity respectively. The measurement of agreement between predicted and measured PAEE will be assessed for Part I and II of the study using the Bland-Altman statistical procedure. If high measurement of agreement is found between the Actiheart™ and the two criterion measures of PAEE, health researchers will gain an additional tool for the assessment and quantification of human behaviour and physical activity.
Background Information/Introduction
The Actiheart™
The Actiheart™ is a device worn on the chest, attached by two adhesive electrodes. This device simultaneously collects data on real-time heart rate and movement counts (movement counts being a quantification of the amount of acceleration an individual’s arms and legs produce during activity). Heart rate and movement count data are collected at an epoch of 15 seconds and is stored within the internal memory of the device. These data are downloaded from the Actiheart™ onto a computer. Then, using computer software and specific equations provided by the manufacturer, an overall measure of an individual’s total PAEE is calculated. The combination of physiological data with movement sensing is predicted to increase precision to our current methods for measuring PAEE. (See diagram below as to how the Actiheart™ attaches to an individual’s chest)

The Actiheart™ attaches to the chest by two adhesive electrodes. One electrode is placed on the sternum at the level of the third intercostal space. While, the second electrode is placed adjacent to the first somewhere on the major Pectoralis muscle. Electrodes need to be replaced every couple days, or as they become unadhesive due to perspiration, being dampened in a shower, etc.
Indirect Calorimetry (Part I)
Indirect calorimetry estimates energy expenditure via the measurement of oxygen consumption and carbon dioxide (CO2) production. The more intense an activity is or the more active an individual is, the greater the amount of oxygen is consumed and the greater the amount of CO2 is produced. Thus, the more energy one will expend. For PAEE measurements using indirect calorimetry, an individual must be suited with a ventilation mask. The ventilation mask is hooked up to a gas analysis machine called a metabolic cart which analyzes the amount of oxygen an individual consumes, as well as the amount of CO2 an individual produces. In order to obtain accurate measures of PAEE, an individual must wear the ventilation mask for the full duration of the exercise (or activity) energy expenditure is being measured. This type of measure provides a very accurate measure of PAEE. However, a major limitation is that it is only practical for use during lab-based activity. (See diagram on how an individual is hooked up to indirect calorimety machine). 
This is a picture of a COSMED Quark b2 indirect calorimeter ventilation mask. With indirect calorimetry, an individual is fitted with a similar rubberized gas mask as shown here. This mask is directly connected to a machine by tubing which will analyze the total amount of oxygen one consumes and the total amount of carbon dioxide one produces while performing a certain type of activity (e.g., treadmill walking).
Doubly Labeled Water (DLW) (Part II)
DLW is a liquid mixture containing the two stable isotopes deuterium (²H) and oxygen-18 (O18). Deuterium is an isotope of hydrogen (H2) and oxygen-18 an isotope of oxygen (O). Stable isotopes are not radioactive and only differ from the common elements (in this case hydrogen and oxygen) by having a slightly heavier atomic mass. Atomic mass is the total mass of all protons, neutrons and electrons bound together forming a single atom. (See diagram below). Both the stable isotopes deuterium and oxygen-18 are found in natural abundance in the earth’s oceans, as well as naturally in trace amounts within the human body.
With DLW, small doses of deuterium and oxygen-18 (comparable to an amount normally present in the human body) are required to be consumed by an individual. Once absorbed by the body, the DLW molecules stabilize and balance with existing total body water. Deuterium and oxygen-18 water molecules act as metabolic tracers. By tracking the elimination rate of deuterium and oxygen-18 from the body, one can calculate total carbon dioxide (CO2) production and thus can calculate the total amount of energy one has expended over a given time frame. The most common way to track the elimination rate of these two isotopes is through urine. Using isotope mass spectrometry, urine samples can be analyzed and thus the quantification of how many DLW molecules metabolized by the body for a given time period. Urine samples must be collected directly before as well as five hours following a DLW drink to determine baseline measures of deuterium and oxygen-18. In addition, urine samples are collected from the second and last voids of the first, mid, and final days of the time period energy expenditure is being quantified. These additional urine samples are used to track the rate that deuterium and oxygen-18 are being metabolized and eliminated from the body. By tracking the elimination rate of deuterium and oxygen-18, total CO2 production and thus total energy expenditure can be calculated. (Please see diagram below on how deuterium and oxygen-18 isotopes are utilized and eliminated by the human body).

The deuterium and oxygen-18 DLW molecules (²H2 18O) are drank and than equilibrate throughout an individual’s body water. Naturally, an individual’s body must brake down water (H2O à H2 + O) to make the needed energy required for the body to function at rest and in addition to when engaging in activity. Once a water molecule (H2O) is broken down, hydrogen (H2) is predominately eliminated from the body through water (i.e., urine) and oxygen (O) through both carbon dioxide (CO2) and water (i.e., urine). Similarly, as the body brakes down a DLW molecule (²H2 18O à ²H2 + 18O) for energy use, the deuterium (²H2) like hydrogen is eliminated predominately through urine and the oxygen-18 (18O) through both CO2 and urine. By quantifying how much deuterium and oxygen-18 have been eliminated by the body through urine, total CO2 Production, and thus energy expenditure can be calculated. The more active an individual is, the more water ones body must metabolize and greater levels of CO2 are produced.
Currently, DLW is the gold standard for measuring energy expenditure for the activities humans engage in while at rest, as well as throughout their daily lives. It has been widely used by health researchers for calculating total energy expended in adult, adolescent, children, and infant populations. Unfortunately, the high costs associated with the purchasing and analysis of each isotope makes this measure unfeasible, particularly for studies involving large numbers of participants.
Part I - Study Methods/Procedure
Twenty-two adolescents (male = 11, female = 10, mean age =17.29 S.D.=.78 ) were recruited from secondary and post secondary institutions in London Ontario. Individual as well as parental consent was obtained from each participant prior to start of the study. Each participant read and completed a Physical Activity Readiness – Questionnaire (PAR-Q) indicating he or she were able to engage in physical activity, in addition to the completion of documentation pertaining to demographic and contact information. Following consent each participant scheduled a visit to the Exercise and Health Psychology Laboratory (EHPL) to complete Part I of the study.
During the participant’s visit to the EHPL, participant height and weight were taken using a standardized Health-O-Meter. Percent body fat measures were obtained using duel- energy x-ray absorptiometry (DXA). Following the above anthropometric measures, participants were equipped with an Actiheart™ device and engaged in a standard fitness test, where treadmill speed and incline increase incrementally over a 21 minute structured protocol or until volition fatigue was reached. Measured PAEE was obtained using a COSMED Quark b² metabolic cart (see description provided previously re: Indirect Calorimetry).
Part I – Results
Measurement of agreement was analysed between Actiheart™ predicted and indirect calorimetry measured PAEE using the Bland-Altman (Bland & Altman, 1986). See Figure 1. Overall this analysis shows that the Actiheart™ underestimates PAEE by a mean of .03 kcal/min/kg. The limits of agreement were -.06 and .11 kcal/min/kg, i.e., the Actiheart-PAEE value could range from .06 kcal/min/kg below to .11 kcal/min/kg above the indirect calorimetry-PAEE value.
Minute-by-Minute AEE Across the Entire Treamill Exercise

Figure 1 Comparison of the Average PAEE-derived from both Indirect Calorimetry and the Actiheart with the difference between Indirect Calorimetry and Actiheart –derived PAEE.
Part II – Study Methods/Procedure
Following completion of Part I, a return visit was scheduled for the commencement of Part II. In total the time frame participant PAEE was being tracked for in Part II was 9 days. Participants second visit to EHPL was in the p.m. hours, following supper, when they received their DLW drink (Day 0). Upon arrival each participant was given a urine sample container and provided a pre-dose urine sample. Next, a prepared weighted mixture of DLW was given to each participant (the volume of DLW administered was dependant on the body composition data collected during their initial visit to the lab, consisting of 0.15g ²H2O and 0.3g H218O/kg estimated total body weight). Following the DLW drink, each participant was given an additional urine sample container and requested to provide a urine sample 5-hours following the DLW.
Participants returned to the EHPL the following morning (Day 1) in a 12-hour fasted state and a measure of one’s resting metabolic rate (RMR) was obtained via the Cosmed Quark b². Each participant was fitted with a ventilation mask and asked to lie quietly for 30min, while resting respiratory data are collected. Following the RMR measure each participant was re-fitted with an Actiheart™ (the same device that they wore during Part I) and given sample containers for the additional urine collections required over Part II. Collection was required from the second and last voids of Days 1, 5, and 9. Urine samples were stored in a fridge until pick-up. Following each collection day, a research participant collected the urine samples from each of the participants (with the exception of Day 9 collections) and stored them in a freezer at the EHPL until sent away for analysis.
On Day 10, each participant brought there final urine samples to the EHPL where the Actiheart™ device was removed and the information was downloaded and saved off the device. Participants filled out the short questionnaire to assess health enhancing physical activity (SQUASH) pertaining to the previous nine days the Actiheart™ had been worn. Completion of the SQUASH indicated the completion of Part II. Participants were thanked for their involvement in the study.
Part II -Time Line

Part II – Results
Data have yet to be analysed and hence are not reported.
For further information about this study, please contact Nerissa Podolinsky npodolin@uwo.ca
An Integrated Theoretical Approach to Increasing Physical Activity in School-Aged Children
A minimum of thirty minutes in moderate to vigorous PA on most days of the week is suggested for children to accrue psychological and health benefits (Boutcher, Biddle, & Fox, 2000; Centers for Disease Control and Prevention,1996; Warburton, Nicol & Bredin, 2006). However, fewer than half of Canadian children currently meet this standard (Public Health Agency of Canada, 2002) making increasing physical activity an important health objective.
Previous research conducted through the EHPL revealed that self-efficacy measures could accurately discriminate lower active children from higher active children as measured using subjective and objective measures of physical activity. A series of three studies are being conducted to extend this work.
The specific aims of this research program are:
- To create and validate an inventory that integrates basic psychological needs theory and self-efficacy theory for use with school-aged children in free-living PA settings.
- To identify salient variables that will predict objective and subjective PA prospectively.
- To test the ability of an intervention based on salient predictor variables (determined in study 2) to increase objective and subjective PA in school-aged children.
Study 1: SCALE MODIFICATION AND VALIDATION (in progress)
Individual interviews conducted with five school-aged children in study 1 informed item modifications and ensured comprehension of questionnaires. Subsequently, items were incorporated into an item content review form and delivered to experts in self-efficacy and self-determination theories to establish the content validity following our minor modifications.
Study 2: THEORY INTEGRATION AND RELATIONSHIP ESTABLISHMENT
In a 6-week longitudinal study school children (N = 164) will complete questionnaires developed and evaluated in study 1, and will wear an Actical® motion sensor during week 1 and week 6. These accelerometers will objectively assess the energy expenditure of PA, and provide omnidirectional accelerometry data that has shown to possess acceptable reliability and validity in previous energy expenditure measurement studies involving youth. Upon returning the devices, children will complete a subjective 7-day PA recall measure which will provide a description of the specific activities in which they engaged. This will also allow for the validitation of the self-report instrument compared against objective PA data. This study will establish the existence and strength of relationships between integrated model variables and PA, as well as the stability of these relationships over six weeks.
Study 3: INTERVENTION DEVELOPMENT AND IMPLEMENTATION
Variables that show a significant and stable relationship with PA in study 2 will form the basis of a planned PA intervention whereby children (N = 100) who score lower in salient social cognitive variables in study 2 will participate in a randomized trial. A group mediated approach to motivational interviewing with an emphasis on these mediators will form the basis of the intervention. As such, this trial will examine whether manipulating social cognitive variables such as self-efficacy and basic psychological needs variables via a group mediated motivational interviewing intervention will have a positive effect on intensity, duration and number of sessions of PA. As in study 2, this study will also assess PA both subjectively and objectively.
For further information about this research program contact Casey Gray cgray9@uwo.ca
Out of the Blue: Exercise Treatment for Depression
Depression is a common and disabling mental health issue. Depression is often associated with low levels of self-confidence to perform certain tasks (self-efficacy). Also, in those with depression high levels of the stress hormone cortisol are often present, which may affect memory performance through effects on a part of the brain called the hippocampus. Exercise is one depression treatment that has been shown to be efficacious. The purpose of the study was to examine the psychological, cognitive and physiological changes that occur during the course of an exercise program in those with clinical depression.
Depressed participants were randomly assigned to either a six week aerobic exercise (n=10) or stretching (n= 13) program. The outcome variables were depression severity, coping efficacy, episodic memory and cortisol awakening response (CAR), defined as the difference in cortisol concentration between waking and 30 minutes post waking. In both groups, depression significantly decreased over six weeks, accompanied by a decrease in CAR and significant increases in coping efficacy and memory performance.
Change in depression was correlated with change in coping efficacy and change in CAR. Change in episodic memory was correlated with change in CAR. Overall, this study demonstrates that exercise is an efficacious depression treatment and is associated with positive psychological, cognitive and physiological changes.
 Figure 1: BDI scores at baseline and six weeks in exercise and stretching groups. BDI = Beck Depression Inventory, a measure of depression severity
Figure 1: BDI scores at baseline and six weeks in exercise and stretching groups. BDI = Beck Depression Inventory, a measure of depression severity
Predicting Physical Activity Intention and Behaviour in School-Aged Children
Two studies were conducted to predict physical activity in school-aged children. Study 1 tested the utility of an integrated model in predicting physical activity (PA) intention and behavior—the Theory of Planned Behavior (TPB) and Self-Efficacy Theory. Six hundred and forty-five New Zealand children (aged 11-13 years) completed measures corresponding to the integrated model and a self-reported measure of PA one week later. Perceived behavioral control (PBC) and subjective norm were the two strongest predictors of intentions. Task efficacy and barrier efficacy were the two strongest predictors of PA.

A second study (Study 2) was conducted to determine whether the self-efficacy measures could discriminate objectively measured PA levels. Sixty-seven Canadian children (aged 11-13 years) completed task and barrier self-efficacy measures. The following week, children classified as ‘high’ (n = 11) and ‘lower’ (n = 7) for both task and barrier efficacy wore an Actical monitor for seven consecutive days to provide activity-related energy expenditure (AEE) data. Results showed that children with high efficacy expended significantly greater AEE than their lower efficacious counterparts.

Findings from these two studies provide support for the use of self-efficacy interventions as a potentially useful means of increasing PA levels among school-aged children.
Examining the Effect of a Goal-Setting Intervention on Self-Efficacy, Intention and Exercise Adherence in Minority Women
The benefits of physical activity have long been recognized, and regular physical activity has been shown to aid in protecting against various chronic conditions such as type 2 diabetes, cardiovascular disease, stroke, hypertension, osteoporosis, and many others (Canadian Fitness and Lifestyle Research Institute, 2005). Many of these conditions are preventable, and engaging in physical activity is one way in which people might deter the development of diseases which could eventually be fatal. However, despite the obvious risks of sedentary lifestyles and the benefits of physical activity, approximately two-thirds of the Canadian population are not sufficiently active to gain health benefits (Craig, Russell, Cameron, & Beaulieau, 1999). Women are statistically less physically active than men: 47% of Canadian men and only 41% of Canadian women are physically active (Lox, Martin Ginis, & Petruzzello, 2006). Moreover, researchers have concluded that women in all ethnic groups are more likely to be physically inactive (Bryan et al., 2006). This suggests that women belonging to ethnic minority groups have a very high rate of physical inactivity, higher than that of Caucasian women, and thus comprise a very inactive segment of the population.
There is currently a paucity of research on physical activity interventions and specifically the effect of goal setting on adherence among minority women. One purpose of this study was to investigate the effect of a 6-week goal-setting intervention on task, coping, and scheduling self-efficacy. Participants who self-set goals were hypothesized to increase their overall self-efficacy, especially scheduling self-efficacy, compared to those whose goals were assigned. Another purpose of this study was to investigate whether the participants’ intentions to exercise (i.e., increase, maintain and decrease their participation) changed over the course of the 6-week intervention and whether any such changes were related to whether the participants were assigned goals or set their own goals. Since no previous research has examined the relationship between these various types of intentions and goal-setting, no specific hypotheses were forwarded. The final purpose was to determine whether the goal-setting physical activity intervention had an effect on physical activity adherence among minority women. It was hypothesized that participants who were involved in setting their own goals for physical activity duration and frequency would have better adherence during the exercise program compared to those whose goals were assigned.
A total of 97 participants completed the baseline assessment and were randomized into one of three groups. Participants in Group 1 or the short-bout group were required to engage in exercise on five or more days of the week for thirty minutes per day with the option of accumulating the thirty minutes over the day in 10-minute bouts. Participants in Group 2 or the long-bout group were required to exercise three times a week for thirty minutes at a time. Finally, Group 3 or the goal-setting group began exercising at an individually-determined frequency and decided whether to accumulate their exercise in long or short bouts. Their ultimate goal was to exercise according to the ACSM recommendations, five days a week for thirty minutes a day. The 6-week intervention was home-based with all groups engaging in their exercise either at their homes, outside, or at other places of their choosing (e.g., park, gym, etc).
The first purpose of the present study was to investigate the effect of a 6-week goal-setting intervention on task, coping, and scheduling self-efficacy. Participants who self-set goals were hypothesized to increase their overall self-efficacy compared to those whose goals were assigned. This hypothesis was not supported. Between baseline and the end of the intervention, scores for coping self-efficacy increased significantly for all groups. From the baseline measurement to the conclusion of the program, the short-bout and long-bout groups’ task self-efficacy increased while the goal-setting group’s task self-efficacy decreased (see Figure). Also, from baseline to the end of the program no significant changes were evident for scheduling self-efficacy for any of the groups.

Another purpose of this study was to investigate whether the participants’ intentions to exercise changed over the course of the 6-week intervention and whether any such changes were related to whether the participants were assigned goals or set their own goals. The participants’ intentions to maintain, increase and decrease exercise all changed and were in accord with those reported by Milne et al. (2008). Regardless of whether participants were assigned goals or set their own goals, their intention to maintain their current level of activity increased between baseline and the conclusion of the study for all groups. In terms of intention to increase levels of activity, participants’ scores decreased from baseline to the end of the intervention. Finally, participants’ intention to decrease current levels of activity increased from baseline to the conclusion of the study.
The final purpose of this study was to determine if a goal-setting intervention could positively influence adherence to physical activity over the course of a 6-week intervention.
It was hypothesized that participants who were involved in setting their own goals for physical activity duration and frequency would have better adherence during the exercise program compared to those whose goals were assigned. The results revealed that the three adherence measures: frequency, duration, and intensity, all declined over the course of the intervention. Additionally, a significant difference was found for adherence to frequency of activity between the short-bout and goal-setting groups. This would be an expected finding for the beginning of the intervention because the groups were instructed to engage in differing frequencies of physical activity per week. However, in the sixth week, the goal-setting group was expected to be exercising as frequently as the short-bout group, as the goal-setting group’s ultimate goal for frequency of activity was five days per week, the same as that of the short-bout group’s goal throughout the intervention. The goal-setting group never achieved this goal and continued to report fewer days of physical activity per week for all six weeks of the program, possibly explaining the differing frequencies of activity between this group and the short-bout group (see Table).
Table
Descriptive Statistics for Exercise Frequency- Number of Days per Week
|
|
Short bout Group (n=29) |
Long bout Group |
Goal-setting Group |
Total |
|
Week 1 |
3.41 (2.04) |
2.92 (.89) |
2.14 (1.18) |
2.73 (1.52) |
|
Week 2 |
3.21 (1.97) |
2.69 (.88) |
2.05 (1.36) |
2.57 (1.54) |
|
Week 3 |
3.07 (2.30) |
2.85 (1.29) |
2.40 (1.17) |
2.72 (1.62) |
|
Week 4 |
2.52 (2.21) |
2.31 (1.16) |
2.21 (1.55) |
2.33 (1.68) |
|
Week 5 |
2.72 (2.19) |
2.35 (1.44) |
1.67 (1.69) |
2.16 (1.84) |
|
Week 6 |
2.86 (2.31) |
2.23 (1.48) |
2.33 (1.88) |
2.46 (1.93) |
Values are expressed as means (SD).
The present study has various strengths. This investigation is one of only a few theoretically-driven interventions that have examined the effects of goal setting on physical activity participation among minority women (also see Castro et al., 1999; Williams et al., 2008). Also, multiple types of exercise self-efficacy and exercise intentions were considered, providing a more complete understanding of how these self-regulatory variables change over a 6-week home-based exercise program. In addition, the three measures of exercise adherence employed in the present study answer Wareham and Rennie’s (1998) call for the use of objective measures of exercise behaviour.
Self-presentation in exercise: changes over a 12-week cardiovascular program for overweight female initiates
Erin Pearson, Craig Hall, and Kimberley Gammage
In the context of physical activity, self-presentation is defined as the portrayal of a socially favourable impression whereby individuals attempt to monitor and control the perceptions and evaluations of others around them through the presentation or omission of certain behaviors. Self-presentational concerns can materialize for those new to exercise (i.e., initiates) as these individuals may worry that they will be perceived by others as uncoordinated or unfit, or feel uneasy about the appearance of their bodies while exercising or wearing athletic attire. This is especially the case for those initiates who also feel that they are overweight. In exercise psychology research, social physique anxiety (SPA) is a commonly studied aspect of self-presentation. Individuals can experience feelings of anxiety when they are concerned about the prospect or presence of unfavourable, interpersonal, physique-related evaluations by others. Given the high rates of sedentariness among adult Canadians, and the fact that self-presentational dimensions and SPA have been shown to influence exercise behaviour, the purpose of the present study was to examine these cognitions in a sample of new exercisers over the course of a structured, 12-week cardiovascular exercise program.
Participants were forty-nine overweight and obese female non-exercisers [M age = 34.88 years; M Body Mass Index (BMI) = 29.67 kg/m2]. The Self-Presentational Efficacy Scale (SPES) and the Social Physical Anxiety Scale (SPAS) were completed at three time-points (i.e., baseline, 6-weeks, and 12-weeks). The SPES assesses aspects of self-presentational efficacy in the context of physical activity: (1) Self-presentational efficacy expectancy (SPEE) assesses how confident individuals are of performing behaviours and presenting images that lead to certain self-presentational outcomes; (2) Self-presentational outcome expectancy (SPOE) is the extent to which individuals believe that regular exercise will lead to specific self-presentational outcomes; and (3) Self-presentational outcome value (SPOV) measures the importance that is placed on achieving self-presentational outcomes. The SPAS assesses the anxiety levels associated with other people’s evaluations of one’s body. Anthropometric measures including body weight, BMI, and waist circumference were obtained at baseline, and weeks 6 and 12.
Separate repeated measures ANOVAs revealed significant increases in efficacy expectancy, outcome expectancy, and outcome value between baseline and week six; only efficacy expectancy demonstrated a further increase between weeks six and twelve. A significant decrease in SPA between baseline and week twelve was also observed. In addition, bivariate correlation analyses were conducted to determine whether any relationships existed between body composition and exercise cognitions over the 12-week program. Significant negative correlations were found between SPEE and weight, BMI, and WC at all time points. The relationship between SPOE and body composition values revealed significant positive correlations in the latter half of the exercise program (i.e., 6-12 weeks).
Overall, the present study revealed that the completion of a 12-week cardiovascular exercise program can elicit significant changes in body composition, self-presentation, and SPA in a population of overweight and obese women. When introducing an initiate population to exercise, the use of a private facility should be considered, given its propensity to reduce self-presentational manifestations such as SPA. This is especially the case for individuals who fall within the overweight or obese range. Findings of the present study indicate that changes in body composition can impact self-presentational variables positively during an exercise intervention. Eliciting more salient physiological changes near the beginning of an exercise program (e.g., through the addition of a strength training component) may serve to improve and sustain changes in self-presentation while reducing SPA simultaneously. Finally, given that significant changes to self-presentational variables occur generally within the first six weeks of an exercise program, these dimensions should be emphasized in the development and early implementation phases. For example, making modifications to the exercise environment such as removing mirrors, positioning equipment together to promote group cohesion, and privatizing facilities to include exercisers with like abilities and constitutions could serve to enable participants to reach this time point. Similarly, insights into when and how individuals come to place value on self-presentational outcomes would be of benefit. Once these thresholds are determined, interventions can be tailored to assist participants in reaching these points, thus potentially improving long-term adherence rates.
Descriptive Statistics for the Self-Presentational Efficacy Scale and the Social Physique Anxiety Scale by Administration Time Point (n = 49)
|
|
Baseline |
6-Week |
12-Week |
|||
|
Measure |
M |
SD |
M |
SD |
M |
SD |
|
SPEE |
26.82 |
17.63 |
40.80 |
21.77 |
45.39 |
24.60 |
|
SPOE |
2.66 |
1.08 |
2.88 |
.95 |
3.03 |
1.05 |
|
SPOV |
3.06 |
.98 |
3.37 |
.89 |
3.32 |
.95 |
|
SPAS |
3.02 |
.61 |
2.81 |
.67 |
2.79 |
.67 |
For further information about this trial, please contact Erin Pearson at ecrooke@uwo.ca
The influence of body weight information on exercise motivation in non-exercising, overweight women
Erin Pearson, Craig Hall, Wendy Rodgers, and Philip Wilson
In today’s society, ideals of attractiveness and a thin appearance often serve as motives for a lifestyle behaviour change such as exercise. While making an effort to meet these ideals; many individuals weigh themselves daily in the hopes of observing a decreased scale weight. However the reality, especially for women, is that daily fluctuations in weight are virtually unavoidable. Reactions to weight fluctuations during exercise are multi-faceted and can include a decrease in exercise cognitions such as motivation; an important determinant with regards to predicting adherence. Although the health related benefits of exercise may be apparent shortly after commencing an exercise program, physical activity has been identified as a slow and challenging method for improving appearance. Subsequently, many women focused on weight loss are often set-up for disappointment which can perpetuate low motivation to engage in physical activity and poor adherence to an exercise regime. Accordingly, a unilateral focus on scale weight during the initiation of physical activity may not be the best indicator of success. There has been some evidence that individually-tailored information within an intervention can elicit significant health behavior change. When considering the design of an exercise intervention, little is known to date about the relationship between exercise and the provision of personalized body composition information and scale weight on exercise motivation. Therefore, the purpose of the present study was to examine the impact of providing individualized body composition information obtained by Dual Energy X-Ray Absorptiometry (DXA), versus body weight information only on exercise motivation. This occurred during a baseline assessment for overweight and obese female non-exercisers, intending to begin an exercise program. As weight-loss has been identified as a common motivator for initiating an exercise program, it was hypothesized that the supplementary provision of body composition information would enhance motivation to engage in exercise.
Participants were 80 overweight and obese female non-exercisers between the ages of 19 and 45 (M Body Mass Index = 29.02 kg/m2; SD = 4.7). The Behavioral Regulation in Exercise Questionnaire-2 was completed as a measure of motivation prior to and following the provision of the body composition or body weight information. Overall, results revealed that for overweight women new to exercise, providing body weight information produces an immediate decrease in all forms of exercise motivation, and this is more pronounced for those women with higher body fat. Moreover, if body composition information is also made available, this decrease in motivation is attenuated significantly. Research and fitness experts seeking to enrol female initiates in physical activity should avoid the immediate provision of, and emphasis on body weight, particularly if the initiates are overweight. If body weight information is given to these individuals, also providing them with body composition information may serve as a buffer for the impact of body weight information on their exercise motivation.
For further information about this trial contact Erin Pearson at ecrooke@uwo.ca